

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¶ Welcome and CardioNerds Mission
worldwide cardiovascular disease affects the lives of hundreds of millions dedicated cardio nerds everywhere are working hard to fight this global epidemic these are their stories Welcome back CardioNerds. Thanks for joining us as we tour fellowship programs across the country. As part of the CardioNerds case report series produced in collaboration with the ACC fellow in training section, each episode will feature a cardiology fellowship program.
Fellows from the program present and teach about a fascinating case and share what makes their hearts flutter about their program. Each case discussion is followed by an eCPR segment from a content expert and a message from the program director.
Before we dive in, just remember, we are an independent educational platform. This podcast is not meant to be used for medical advice. The views expressed here do not necessarily reflect the opinions or policies of our employers. The case you are about to hear is 100% HIPAA compliant.
We thank you for subscribing to and supporting the CardioNerds. Our mission is simple, to democratize cardiovascular education, promote diversity and inclusion, empower everyone to learn and teach from the basics to the advanced while fostering wellness and humanity. If you believe in the mission, consider supporting us on patreon.com slash cardio nerds. Every little bit goes a long way. We're also so excited to be growing the platform by mentoring the next generation of cardio nerds.
We are establishing the CardioNerds Academy and are looking for residents and fellows to join as CardioNerds fellows. Please see the link in the episode description to submit an application. Without further ado, let's continue on our tour with another fascinating case from amazing...
¶ Houston Methodist Fellows Introduction
CardioNurse colleagues. We are back and so excited to be with our colleagues here in the beautiful city of Houston. We're joined by Dr. Stephanie Fuentes, Peter Rothstein, and Isaac T. fellows from the Houston Methodist Cardiovascular Training Program. Guys, welcome to the show. Would you please introduce yourselves?
Morning, I'm Stephanie Fuentes. I'm one of the second-year cardiology fellows here at Houston Methodist. I was running Peru. I did my medical school at UTMB and continue on for residency and fellowship here at Pursuing Aertrophysiology Subspecialty. And my name is Peter Rothstein. I'm one of the third year cardiology fellows here at Methodist. I did my residency at University of Colorado, and I'm originally from Milwaukee, Wisconsin.
Like Stephanie, I'm also going into electrophysiology, applying right now. I'm Isaac T. I'm the third year cardiology fellow, also the chief fellow here at Houston Methodist. I am myself, I'm originally from Singapore, came to the United States to pursue my clinical training.
I did my internal medicine over at the Lake Canal Medical Center in Philadelphia, but decided I need warmer weather. So I'm here now in Houston. I'm starting my interventional fellowship next year here at Houston Methodist as well. Hopefully with my co-fellow Peter here, who will be by my side doing EP at Houston Methodist as well. Wow, that's great. Isaac, Stephanie, Peter, welcome to the show.
We are so excited to be here in Texas. And I have to say, you know, having people from Houston do residency where I'm at, I definitely saw a high percentage of people that wore all out boots. under their scrubs. Is that a real thing? Do people do that in Houston? Yes, it is. You know, I didn't see that in Colorado ever, but I see it on a daily basis here in Houston. So, you know, I actually bought a pair of boots and I moved down here.
Only the clinic. It's more of a dressy thing. I'll say a shout out to Tommy Daz, who's a resident producer for this episode and was from Houston. He often... attended our bedside rounds with cowboy boots on, and I loved it. We all loved it. Absolutely amazing. So I'll put questions about sweaty feet aside, because I'm right now wearing flip-flops, so it's neither here nor there.
Could you guys take us to your favorite chill spot in Houston and have a great discussion about cardiology? Where are we going, guys? I guess we could go to Herman Park. It's close to the med center. It's a relaxed area. It's family friendly and dog friendly as well. Yeah, Herman Park's a great place. They've got tons of birds and flowers and fountains, and it's a nice outdoor space.
Herman Park. Guys, this is Labor Day weekend while we're recording. It's a beautiful Sunday outside. I can't imagine a better place to be to celebrate our Labor Day weekend on a Sunday morning. We're here. We're taking in the breeze. We're hanging out. Let's do what we love to do. Talk about cardiology.
¶ Patient Presentation and Angina Workup
What do you have for us? All right, we'll get started. This is a 71-year-old gentleman with coronary disease for which he underwent a PCI proximal LED back in 2016. And he came into clinic with worsening angina and dysmium excursion for about one month, despite being on anti-anginal medical therapy. He had a nuclear stress test that showed abnormal myocardial perfusion, consistent with a large, severe ischemic defect in the RCA territory.
And his other medical history, other than the coronary disease, was hypertension, hyperlipidemia, and diabetes. His medications included aspirin, Plavix, Grastor. corvidalol, and lollipine, in addition to his other anti-angelo medications, including isosorbide mononitrate, Ranexa, and lisinopril. He had no contributory family history. He was a former smoker of 40 packs per year, and he had occasional alcohol use.
He had an echocardiogram one year prior to presentation that showed an ejection fraction of 60% with normal ventricular size and function.
¶ Understanding Stress Testing Modalities
He had no hemodynamically significant valvular pathology. Yeah. So Stephanie, this is a great presentation so far. I think we come across this all the time where a patient is coming in with what sounds like angina complaints, and we definitely don't want to miss angina, but there's also a wide differential. the get-go. Thankfully, at this point, we have a patient who has a positive stress test, and so it's already cluing us into the underlying cause of his symptoms.
Initially, before the stress test, we say, okay, these symptoms maybe have classical angina with a chest pressure or other, you know, shortness of breath that is exertional in nature. But he also has... risk factors that increase the likelihood that this is a coronary ideology, hypertension, hyperlipidemia, type 2 diabetes. And it sounds like he has a history of CAD as well with a prior PCI. And so this is a host that's likely to have coronary disease, has risk factors for coronary disease.
And this is a presentation based on the symptomatic perspective that sounds like it could be coronary in nature. And so the next step in risk stratification here was essentially non-invasive testing because it sounded like their pretest probability was neither extremely low.
or extremely high. If the pretest probability was extremely high, I imagine we would have taken the patient directly to the table of truth to get a coronary hensiogram. But here we decided to do a stress test. And so just to break down a stress test, we want to see if there are physiologic changes that aren't present at rest.
but are present in some sort of stressing state. And so there are two components here, right? You need one, a stress factor, and then two, a way to objectively assess a physiologic change. And so the stress factor could be exercise, which probably is the most useful because it's more physiologic.
can give us other indices of risk assessment, like the exertional capacity based on their METs. But then there's also pharmacologic stress, which could be vasodilator stress, which may cause coronary steel away from an area that has a fixed stenosis. or inotropic stress with a butamine that essentially makes the muscle work harder. And so you may not have enough coronary flow reserve to meet that demand. And so on one hand, we need...
a stress factor. And on the other hand, we have to have a way to objectively assess this. The simplest of symptoms, do you provoke the symptoms? That's one thing, but it's not sufficient. The second thing is an EKG, right? And so almost every stress modality will have an EKG by their reversible EKG changes as to depressions and or increasing ectopy.
And in addition to that, we can add on imaging, right? And the imaging modality can be different things. So you can have echocardiogram to look for reversible wall motion abnormalities, nuclear perfusion testing to see if there is perfusion defects in radio isotope tracers.
that have differential perfusion in resting versus the stress state, and cardiac MRI to see if there is a perfusion defect with stress. Specifically within perfusion defects and nuclear testing, there are three options, right? A, there is adequate perfusion at rest.
and adequate perfusion at stress. And so we would say that's a negative study. B, there's adequate perfusion at rest that goes down with stress. And we'd say that's reversible perfusion defect. And so that would be equivalent to ischemia. And C is if there is a resting perfusion defect that persists during the stress state. And so in that situation, either that area is infarcted, it's dead, it's scarred, or it's hibernating.
and potentially viable. And so the viability testing could be useful. And then D is there is inadequate perfusion at rest and there is adequate perfusion at stress, which is not a physiologic scenario and essentially indicates some sort of artifact. Again, just to rewind. This patient comes in with symptoms that are concerning for angina or coronary etiology. There is a whole complex of risk factors, so we know that this is a high-risk host.
Based on an intermediate pretest probability, we did a non-invasive stress test that has a component of a stress factor as well as objective assessment for physiologic change. That's fantastic, Amit. And I'll just add, just to dive a little bit deeper into the modality of imaging that you're using to look at the myocardium as you interrogate.
this heart for ischemia. You really want to know the gist. You may not know all the technical details of the modality, but you want to know the gist of how it works. So just two short examples that highlight. the nuances of stress testing. So for example, if you chose your stress to be exercise and you have your patient exercise on a treadmill, and then you go and now you say, I want to look at what the heart looks like before and after stress.
You could, let's say, choose a stress echo. So what you're going to do is echo your patient right before they get on the treadmill. And then you're going to echo the patient after they get off the treadmill at their peak heart rate. And what you're going to say is, what are their heart walls doing? before and what were their heart walls doing after their peak exercise and then what do the heart walls look like when they recover.
And what we're doing is we're taking advantage of the fact that the blood vessels to the heart have distinct territories. The right coronary artery, the LAD, and the left circumflex all perfuse different aspects of the walls. And so you're going to look for differences in the wall motion. during the stress test so if you have let's say anterior wall that was normal functioning during the rest exam and now at peak exercise that wall is not moving well
but the other walls remain moving well, then you have isolated the territory to an LAD distribution. And that prompts you to think about ischemia in that way. So again, in the echo stress test, you're looking at wall motion. And so you're actually looking at what changes with wall motion from rest to exercise. But conversely, when you think about nuclear stress testing, this is different. In nuclear stress testing,
For the main part, you're not actually looking at wall motion per se, although there is an aspect of stress testing that you do. But what you're actually looking at is perfusion. You're using the nuclear study to demonstrate perfusion to particular territories. The way that it looks at each other, unlike in stress echo, where you're looking at each individual wall and asking if it's.
normal motion, less normal motion, or no motion. In perfusion, you're actually comparing it to the other walls. So in a case where you have one artery that's down, like the LED, you're going to see that the perfusion to that anterior wall is going to... be less at stress than the other walls when they're also being stressed because the right coronary artery and the circumflex artery have perfect perfusion.
If you have a situation, like I'll describe, a patient that I recently cathed who had really classic symptoms. but was on the younger side. And so the primary care doctor thought, you know, maybe this patient should go non-invasive stress testing first. He's really young, doesn't have a lot of other risk factors. The story's good. So I'm going to take it seriously.
So his stress nuclear study was actually totally normal. And we thought that we're going to be caffing at the table of truth. We thought we'd be seeing a completely normal angiogram. But it turned out... that again, the guy had classic stories. His right coronary artery was totally occluded, probably chronically. And his left main artery had a very tight 90% stenosis. And so if you think about it,
All of his myocardium got ischemic out of stress. During non-stress, he was okay, but when he went on the treadmill... All of his myocardium gut stress. And so since the nuclear study looks at the right coronary territory, the LAD territory, and the circumflex territory all at the same time and asks which one is getting perfused better to tell you which one is not getting perfused well, it will...
tell you that all of them are equally getting perfused. And so that's what we call balanced ischemia. And that's a phenomenon that happens by nuclear stress testing. Yeah, Dan, that's such an important point to reiterate. Clues to balanced ischemia would be transient ischemic dilatation.
where with stress, rather than the LV contracting more strongly, the LV cavity actually dilates and there's an EF drop. So that would be a really important clue on SPECT imaging for the possibility of balanced ischemia. And not all nuclear studies are created equal. Pet breast stress has much greater resolution and is less likely to be affected by balanced ischemia and give a false negative in that context.
¶ Cath Lab Findings and Post-PCI Changes
So we're at a point essentially where we have a patient who has anginal symptoms, risk factors, and now has a positive nuclear perfusion imaging, rest stress with reversible RCA territory ischemia. What did we do next? So we brought the patient to the cath lab.
to undergo a left for cath for further evaluation. On arrival, he had an 80 kg that showed normal sinus rhythm with a ventricular rate of 65. He had isolated two-wave inversion, ABL, and had poor R-wave progression, but otherwise normal intervals and no Q-waves. He had a left for calf that showed a luminal irregularities in the left main. Peyton stands in the mid-LED into the Diag 1 with diffuse disease. He had moderate stenosis in the osseal segment of the first OM.
And notably, he had severe eccentric serial stenosis in the proximal to mid segments of the RCA. The decision was made to undergo a PCI of the RCA, given a worsening angina, despite being on maximal anti-anginal therapy and the abnormal myocardial perfusion test. underwent PCI to the proximal and mid-RCA, and the final angiography revealed no evidence of dissection or perforation. There was TIMI-3 flow without any residual stenosis. He was subsequently transferred to the PACU, and he did...
Well, he was observed overnight, and he was symptom-free. Then at 3 a.m., the nurse called the on-call fellow regarding barycardia. At that point, the patient reported mild lightheadedness. He had no chest pain or any other symptoms. Notably, he had no bleeding from the radial axis. And so the uncle fellow goes on to examine the patient.
Vitals were notable for bradycardia with a heart rate of 40, hypotension with a blood pressure of 80 over 58, and tachypnea with a respiratory rate of 22. He was saturated 98% on room air. And the rest of the physical exam was notable for a JVP of 12. He had no discernible murmur or gallops, a mild bivascular rails, and one-plus bilateral lower extremity edema up to the mid-shins, and notably cool extremities. So...
¶ Post-PCI Hypotension Differential Diagnosis
You know, if you're the on-call fellow in the middle of the night and you get called for a post-PCI patient who is now hypotensive, bradycardic, essentially unstable. There's some things you want to immediately go through your mind. Is this a PCI in the context of STEMI or is this a PCI that sort of was in the context of stable angina done for symptoms?
Key things to be looked for, you know, commonly this could be just a vagal event from sheath removal. When was the sheath removed? Was this a femoral access? Was this a radial access? You always want to think about bleeding. So especially for your femoral cases, you want to think about, could this be an RP bleed?
Further complicating this could be dehydration. You know, is this a late case? Is the patient NPO for potentially 12, 18 hours, which happens sometimes? Could this be an allergic reaction to contrast if it's very shortly or immediately after the cath? You want to consider the possibility of acute stent thrombosis, so usually accompanied by chest pain. This could be a coronary artery dissection. It should be difficult to assess at the bedside, but you can get stent edge dissections after PCI.
You have to think about, could this be a coronary artery perforation? When you're putting wires into the coronary artery, you can potentially perforate the artery, which can lead to tamponade. want to look for signs of tamponade. They have elevated JVP, hypotension, or the tachycardic. And then you also want to think about other things like transient coronary artery vasospasm, coronary no reflow, which is more of a...
process of the microvasculature. And then in your STEMI patients, you also have to think about mechanical complications of STEMI. So you want to think about, could this be a VSD, a pap muscle rupture, LV free wall rupture? All these things might have different exam findings, VSD. You'd probably hear a murmur. A pat muscle rupture would lead to severe mitral regurgitation, which may not have as prominent of a murmur. And then a free wall rupture could lead to tamponade once again.
Another complication could be just the access side. So you want to assess the access side for bleeding, hematoma, AV fistula, you can get pseudoaneurysm. or RP bleed. So a lot of these would be more common with the femoral axis site, radial axis site negates a lot of these problems. And also you got to keep in mind, all these patients are going to be on dual antiplatelet therapy.
potentially heparin, potentially other blood thinners. So bleeding would be a main complication you'd want to worry about for hypotension post-cath. So those are all things that have to be in your mind on the way to examining the patient. Wow. So that was amazing. And if I could summarize, so basically what you're teaching us is you want to know who's the patient? Why did they have the procedure? What was the procedure?
the access sites and details of the procedure. And then when you develop your differential diagnosis, which you're going to quickly assess, you're going to think about coronary failure related to the procedure, mechanical complications, depending on the situation, and tempanade kind of working your way through.
different components of the heart, or you're thinking about a vascular complication at the access site or anywhere along the pathway, or even at another site unrelated to the procedure, but more related to the systemic anticoagulation. Like, I think that's phenomenal. I just throw out a crazier case that I had going along that algorithm. I had a patient who was post-PCI develop severe abdominal pain.
and ended up having a newly diagnosed hemorrhagic ovarian cyst that was actually expanding that ultimately was followed conservatively. But that was noted on CT as part of why she was having the severe abdominal pain and likely attributed to anticoagulation.
This is like fantastic, fantastic overview of what I would do when I approach a patient post-PCI and I may have been covering and maybe only peripherally involved and now I need to get centrally involved. So thanks for that. That was a great differential for post-PCI shock for hypotension.
¶ Bedside Exam and EKG RV Infarct
How did you evaluate this at the bedside? What's going on in your mind? Yeah, so at the bedside, you have to quickly examine the patient because they're unstable, they're hypotensive. And in this case, he's actually britochartic, not tachycardic, which is concerning.
But you want to do a few things. You want to put your hands on the patient's legs, you know, as high as even the thighs. See, are they cool or are they warm? So essentially, are they perfusing? A really good bedside exam skill is to assess JVP.
And you want to know, is the JVP up? Is it flat? Is it bounding? You want to assess the pulse, any irregularities in the pulse. Potentially it could have arrhythmias post-PCI. You want to listen to the lungs. Do they have rails? Are they breathing okay? Are they wheezing?
Are they having any respiratory distress? Do they have muffled heart sounds, which could potentially be a new pericardial effusion? Do they have any new murmurs? Sometimes after a PCI, you can get ischemia to the pap muscle, which could cause even just transient mitral regurgitation.
You could also have more serious murmurs like a VSD. Another really useful tool is just your 12-lead EKG. It can answer a lot of questions. It can rule some things out. Notably, in someone who just had an RCA stent put in that day, I'd be worried about acute stent thrombosis. So in that case, you would see ST elevations and the inferior leads, 2, 3, and AVF. This was a dominant right coronary artery, so it supplies the PDA, so it supplies the inferior wall.
You could also look for new onset arrhythmias, heart block. Potentially, you could infarct the AV nodal artery. The AV nodal artery comes off the dominant artery. Some people define dominance by what supplies the PDA. Another way of defining dominance is what supplies the AV node. Of course, those are usually the same artery. So you could look for potentially high-grade AV block, complete heart block. You could look for junctional rhythms, sinus node, or rests.
The sinus atrial nodal artery, it's more variable than the AV nodal artery. So it can come off the RCA, come off the circumflex, can come off of both. It can even, in rare circumstances, even come off the aorta. Any new arrhythmia would be concerning, any ST elevations, but you want to notice territory. In our case, what was surprising is a patient at ST elevation in V1 through V4, which was...
confusing because that's typically your LAD territory. A good thing to keep in mind is you have this patient who basically had a PCI not in the setting of STEMI. It was actually in the setting of worsening stable angina. And on the cath films, when you go back and review them, there's actually some large RV marginal branches that were essentially jailed, which is a term we use to say we place stent over the origin of those arteries and essentially occluded those arteries.
So the distal main RCA and PDA had good flow, but the marginal branches did not, which usually does not cause a problem, but in this case can cause poor flow to the RV free wall. And in that setting, you can actually get ST elevations in commonly V1 through V3, but all the way to V4. So this would be your STEMI EKG for an isolated RV infarct, which you can get.
Probably clinically most commonly is the setting when you essentially jail the RV marginal branches. Outside of that setting, it's either you have to have an infarct and an RCA that's non-dominant, so it does not supply the PDA. Essentially, it just supplies the RV free wall.
Or you can actually get STEMI in just a large marginal branch. There's a lot of case reports describing this pattern EKG where ST elevations in V1 through V4, V1 through V3. And then to confirm it, you can get a right-sided EKG. The normal EKG, the only precordial lead that's on the right side of the sternum is V1. So if you want to take a better look at the right side of the heart, easy way would just be to switch V4 to the right side V4 in identical position.
¶ Understanding RCA Side Branch Jailing
And ST elevations there would confirm your suspicion of an RV infarct. Wow, this is incredibly helpful. And folks, I definitely recommend you checking out the blog post for this episode and seeing all of these images and scrutinizing for yourself the before and after pictures of this coronary angiogram.
And then secondly, I just wanted to further clarify about the term jailing. You know, jailing, you can imagine like bars basically crossing over as you stent and... there's a bifurcation or another vessel that's coming out from the main vessel that you're trying to stent, if you put a stent across it, you are going to jail that artery.
just because you jail the artery doesn't mean that there's no perfusion to that artery that you jailed because remember the stents have struts and the struts have holes and blood flow can go down the hole but if you think about the plaque that you're fixing so imagine you have a bunch of calcified but also non-calcified
gooey, ugly, disgusting, fatty plaque, right? When you smush down your stent, right? Remember, you're not roto-rooting the artery. You're really just like displacing all the plaque and smushing it into the wall and basically kind of making a sandwich between the stent and the artery.
If some of the plaque moves over and gets in the way of the branch that was coming up, that would not only result in jailing, but then you could also occlude your artery. Now, in this case, as we just talked about so eloquently, acute marginals.
generally are not a problem for jailing. And, you know, you could theoretically do all these bifurcation techniques to preserve the acute marginal artery, but bifurcation stenting, long-term patency is not as good as straight up stenting, just stenting the main artery. And since most people tolerate these very well, you're not usually going to pursue a bifurcation strategy when it comes to the acute marginal arteries. So that's why that wasn't done here.
But again, just to reiterate the point, just because you stent across an acute marginal doesn't mean you're going to take it out. It sometimes depends on the plaque nature that you're squishing and also if there's disease in the acute marginal branch as well.
That's absolutely right. And I think that's sort of why these cases are tricky, because when you see ST elevations in V1 through V4, you know, you're immediately thinking this is an LAD infarct. What happened? You just had a procedure, but everything was done on the right side.
Everything in the left looked okay in angiogram. So you really have to go back and look at those films yourself and just keep in mind that this could be an isolated RV infarct or at the bedside, you know, you could get a right-sided EKG.
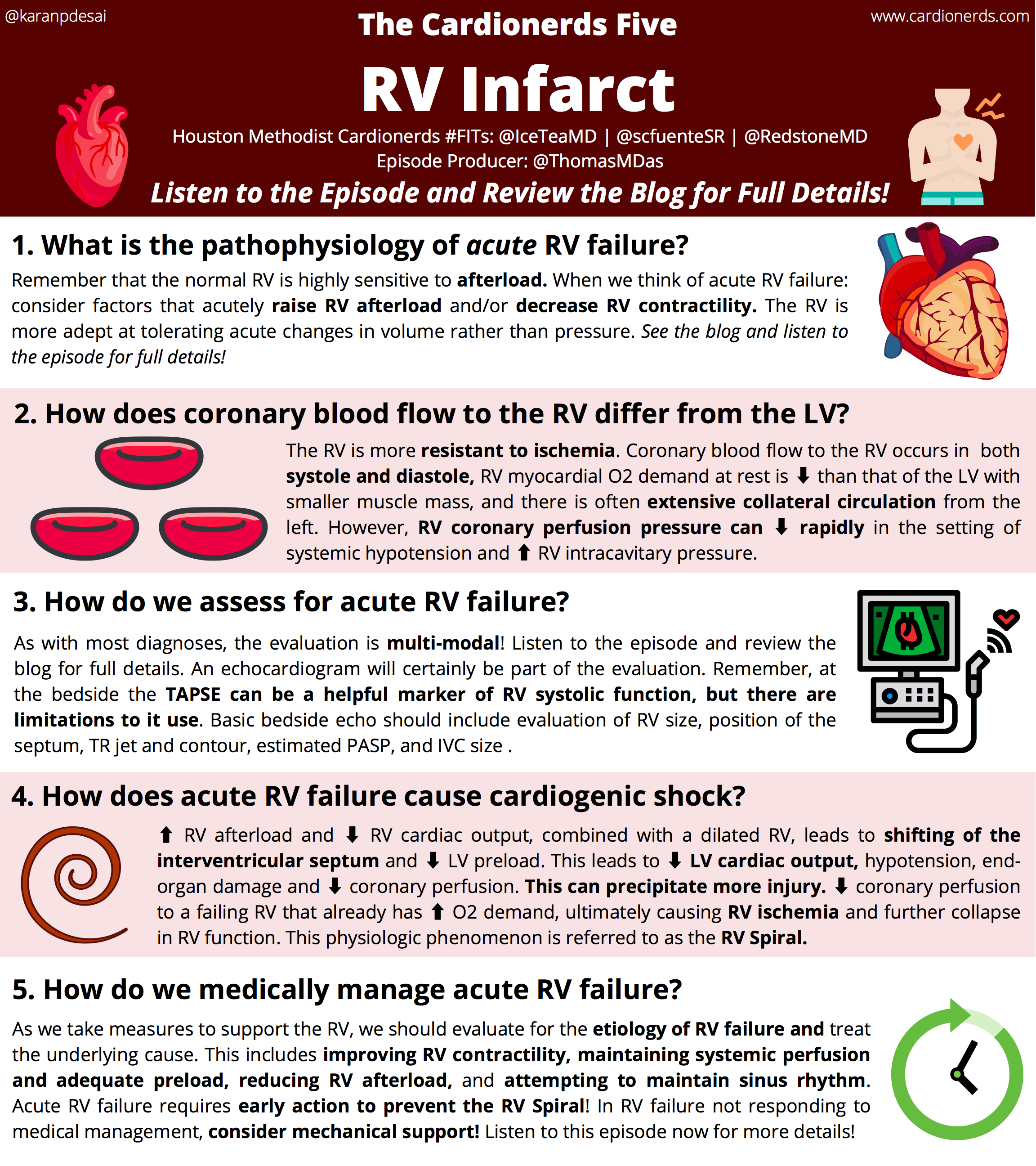
These are great points. And thanks for going over the typical signs of an RV pattern on the EKG. The RV is an anterior structure. It's a right-sided structure. So it stands to reason that when it's injured, you'll have ST elevations in the anterior leads, V1 through V3, maybe even V4, as well as AV. And if you do a right-sided EKG, V3R and or V4R. But just to reiterate, the ST elevation is just an injury pattern. You know, it's not one-to-one equivalent to coronary occlusion.
and ischemia slash infarct. And so this injury pattern we can see in a number of different states. And just to reiterate, the case that we heard from Cedars-Sinai was a patient presenting with essentially an RV pattern current of injury. And the patient essentially had a bradycardic arrest that was later found to be because of a massive pulmonary embolus causing acute RV overload. Clearly in this situation, we know that we lost acute marginals, but I think the two points here are...
to recognize the average pattern of injury and then to also recognize that injury for as the elevation goes beyond just the coronary etiologies. So you raised some great points about side branch occlusion, and really the data that we have is about 19% of cases in which a stat is placed. Across a major, about more than one millimeter of side branch, in most cases, 50% stenosis had already been present at the ostium of the side branch.
Most occlusions occur after post-stent dilation, performed with high pressure inflations. But from this study by Koo in 2005, almost no sidebunch lesions less than 75% visually, and an FFR of less than 0.75. So... they were really not functionally significant. And from this study, among 73 lesions with more than or equal to 75% stenosis, only 20 of them were functionally significant. By six to nine months, usually all branches in these reports, including those previously
occluded or patent. And there was very low morbidity in this series, which reflected a tendency to avoid step placement across large or diseased side branches. which is why we don't always provisionally stent, especially for an RCA acute marginal branch. So going back to the bedside.
¶ Acute RV Failure and Cardiogenic Shock
Because of the physical exam and the EKG findings, the patient had a bedside echo that showed a normal LV ejection fraction of 50-54% with elevated LV filling pressures. But notably, he had a severely enlarged RV. with severe depression with a topsy of 1.4 centimeters. And given the aforementioned physical exam and the EKGN presentation overall, this raised concern for an isolated RV infarct with cardiogenic shock from RV failure.
So at the bedside, the patient received a normal saline bolus of 1.5 liters with transient improvement in blood pressure to 102 over 64. And while he received atrophy initially, he was then started on dopamine to sustain.
¶ Utility of Swan-Ganz Catheter
Harvey. He was transferred to the CCU, and then the consideration for a sworn guns got to the placement of court. Yeah, so this is always a question, right? It's a very good management there, Stephanie, but... then we always come up with the question, does the patient really need a SWAN-GANS catheter? There's gotten a lot of bad press over the years.
from the Pac-Man and escape trials. But if you think about it and you really dig down deep, those trials were not worthless, but they never really studied cardiogenic shock patients. The ESCAPE trial hit 433 patients hospitalized for acute decompensated heart failure to therapy guided by clinical assessment or with a pulmonary artery catheter or by clinical assessment alone.
And they showed that at six months, there was no difference in days alive, out of the hospital or mortality. But the big issue here is... You know, these patients were not blinded, only patients with clinical equipoise, and therefore in patients in whom clinicians felt comfortable managing their heart failure with or without PAC were chosen, and exclusion of the most critically ill and those being evaluated for assist devices.
origin heart transplant. These patients were not included. They did not evaluate the pulmonary artery catheter-guided analysis of pulmonary hypertension reversibility as a component of heart transplant workup. Clinicians had access to CVP measurements.
even though they did not necessarily have a primary artery catheter, and it was difficult to ensure adherence in these groups. And if you think about this in the cardiogenic shock population, and you look at internal quality data from the embryo matter impeller registry,
In patients with cardiogenic shock necessitating an impeller, you can actually see a survival to explant was improved with a swan-gans catheter use. So basically, the take-home point for this is you need the right patient to use it in, to have the right benefit.
And I think in this case here, you know, it's pretty clear. We need to assess his hemodynamics to see what we want to do next. So when you run into the situation, it's always difficult to decide, should I take this patient back to the cath lab to assess their coronaries? especially in this patient, which sort of has V1 through V4 ST elevations. You might want to check out the left anterior descending artery. Could that be the culprit? But what's really helpful here is your bedside exam.
as well as your bedside echocardiogram. This is sort of where your point of care echo can be really helpful. So if the LV is contracting normally, the walls are thickening normally. Ejection fraction is normal. There's no wall motion armality. And then you have a blown out, dilated right ventricle that's weak. The TAPC is low. We kind of use our clinical discretion and decide this is probably just an RV infarct.
And the LAD seems to not be the culprit vessel. Yeah, that makes perfect sense. An acute clinical decompensation post-PCI with changes in the EKG, taking the patient back to the cath lab is an important part of the decision-making. But you use your... bedside approach and knowledge of what we saw on the post-PCI coronary angiogram to understand this is probably RV failure based on the loss of acute marginals. And so you're taking the patient for invasive human dynamic monitoring and...
ongoing management. And I just love that you reiterated the need for the Swan-Gans catheter. I feel like the utility... of the SWAN-GANS catheter is grossly underappreciated based on very limited data that is frequently not relevant to the care of the CCU patient. So I just, I commend you for highlighting that point. So just one last question about the cath and going back.
So was there a point in the decision-making process where we decided to not go back and, let's say, try to dilate the stent struts and open up that acute marginal? Or was that something that we were never thinking about doing because of the fact that it's an acute marginal and because of the discussion? that we had before. Yeah. So it's more of the latter because with these patients, usually even there's plaque shift. It usually resolves sometimes if not...
in a few hours by a few days. So we didn't think that the acute marginals would be contributing so much to the RV per se, because the RCA is really just like a conduit to the PDA. So it supplies, you know, the inferior septum and inferior wall. And usually in most cases, you know, we don't usually see an isolated RV infarct just from jailing some acute marginals. And this happens day in and day out regularly with PCIs through the right coronary artery.
You know, ultimately, there's got to be a decision made about to take the patient back to the cath lab. We talked about taking them back to look at the LAD based on the EKG injury pattern. But there's also a decision to take them back after you look at the films and you saw there's this. pretty sizable acute marginal that went down, should you go back in and try and open that up. And ultimately, with this isolated RV infarct, usually if you can get them through their infarct, they'll recover.
So bringing them back in to try and restore perfusion in the cath lab, we didn't decide to do that. We tried to get him through this RV infarct and knowing based on what is the normal response to that, hoping he would recover. Wow, that really demonstrates powerful clinical decision-making and also the experience that it takes to take care of complex cardiac patients. What information did we get from this one and what did you guys do next to take care of this decompensating patient?
¶ Hemodynamic Parameters: PAPI and CPO
So there's this concept of how many hypotension and RV failure. Just keep that in mind, okay? So the Swann-Gans catheter went in, and these are the numbers. So you had a CVP of 19, RV of 41 over 15, PA of 36 over 20. with a mean PA pressure of 25, a capillary wedge pressure of 18. At the time these measurements were made, his MAP was 60, and by Fick, his cardiac output was 4.2, index of 1.6, and a cardiac power output of 0.56.
And additionally from that, you can get a pulmonary artery pulsatility index, also known as the PAPI. And what we had here was 0.84. So these numbers are all good and well, but what do they mean? PAPI is a very novel hemodynamic index that's come up over the last 10 years or so that predicts RV failure in the setting of an acute inferior wall myocardial infarction and was developed with the goal of identifying patients who will require percutaneous mechanical...
our VAT support, so MCS for the right side of the heart, is now found in acceptance in the clinical practice, particularly in the management of advanced heart failure and cardiogenic shock, as well as patients with LVATs. And the way to calculate it is very simple. It's calculated as the pulmonary artery pulse pressure, so that's the pulmonary artery systolic pressure minus diastolic pressure, then divided by either the right atrial pressure or the central venous pressure.
And the physiological basis for the papi as an indicator of right heart function is predicated on the pulmonary artery systolic pressure as an indirect indicator of RV contractile function against a given afterload. and a high right atrial pressure as a sign of filling right ventricle. So really, the higher the number, the better it is. And the lower, the more concerning for right heart failure. And the number of less than 0.9 has been studied in the ACS acute MI cardiogenic shock setting.
Just a point to note, however, that the index has multiple determinants and will reflect changes in any of the components of the right heart system. So it could be systemic venous system, the RV function, and the primary circulation. And so by extension, this will vary in different populations.
based on the underlying pathophysiology. And a single PAPI threshold across different patient groups is actually not a valid thing. In LVAD patients, a marker of RV function might give you a PAPI of 2 is actually what they use, rather than 0.9.
So you've got to think about this when you're using the PAPI as well. And then just moving on from that, we also calculated here a cardiac power, which is measured in watts, usually in the formula of cardiac output times the mean arterial pressure divided by 451.
It's a very simple calculation. And this actually uses the physical rule of fluids, where power equals pressure times flow. So the cardiac power, as I said, is the product of simultaneously measured cardiac output and mean arterial blood pressure.
Therefore, by coupling both the pressure and flow domains of the cardiovascular system, it measures your cardiac pumping ability. And this is extension from your cardiac index, because the cardiac index really is an index of cardiac contractility, but rather just a measure of... cardiovascular flow, therefore affected by contractility, vascular stiffness, and resistance, as well as intravascular volume and ventricular filling pressures. And that makes the cardiac power output so powerful.
So it's been studied in the National Cardiogenic Shock Initiative database, and a cardiac power output of less than 0.6 watts is indicative of a hemodynamic compromise and is associated with increased risk of mortality. And in fact, the studies have shown that cardiac power is the strongest independent hemodynamic correlate of in-hospital mortality in patients with cardiogenic shock. And that's why these parameters are so important.
¶ Hemodynamic Profiles in Cardiogenic Shock
So in our patient here, he's clearly in RV failure and cardiogenic shock. Now, the question here is whether is the shock the result of left ventricular failure, RV failure, or BIV failure? And this brings me to the concept of hemodynamic profiles in shock. So we used to categorize heart failure based on systemic perfusion and congestive status using a two-by-two table, warm and wet, cold and wet.
cold and dry, warm and dry. In the modern day, we have the Swankens catheter, and we can do a similar two-by-two construct to define the hemodynamic profiles in cardiogenic shock based on a congestive state using measures of left and right heart filling pressures.
So cardiogenic shock then can be categorized into LV, RV, or biventricular dominant congestion or hypovolemia. And the treatment approaches obviously will need to be tailored for each of these four categories. That's why it's so important to define it. So when the commonly kept wet pressure is 18 or below and the CVP is more than 14, we think of predominant RV congestion and RV failure as the issue rather than just biventricular or left ventricular failure.
And this is very important, as I said, because the management for RV failure specifically is drastically different compared to just LV failure or biventricular failure. So in our patient, he had a capillary wedge pressure of 18 and a CVP of 19. as well as a cardiac par output of 0.56 and a PAPI of 0.84. So putting these together, it all points in the direction of just isolated RV failure, which when you put it in the clinical context of what we've discussed earlier,
becomes pretty clear, and hence the importance, again, of the swan-gans catheter in this situation. Isaac, that was a great explanation of why swan-gans catheters can be extremely useful in these cardiogenic shock patients.
¶ Escalating Medical Therapy for RV
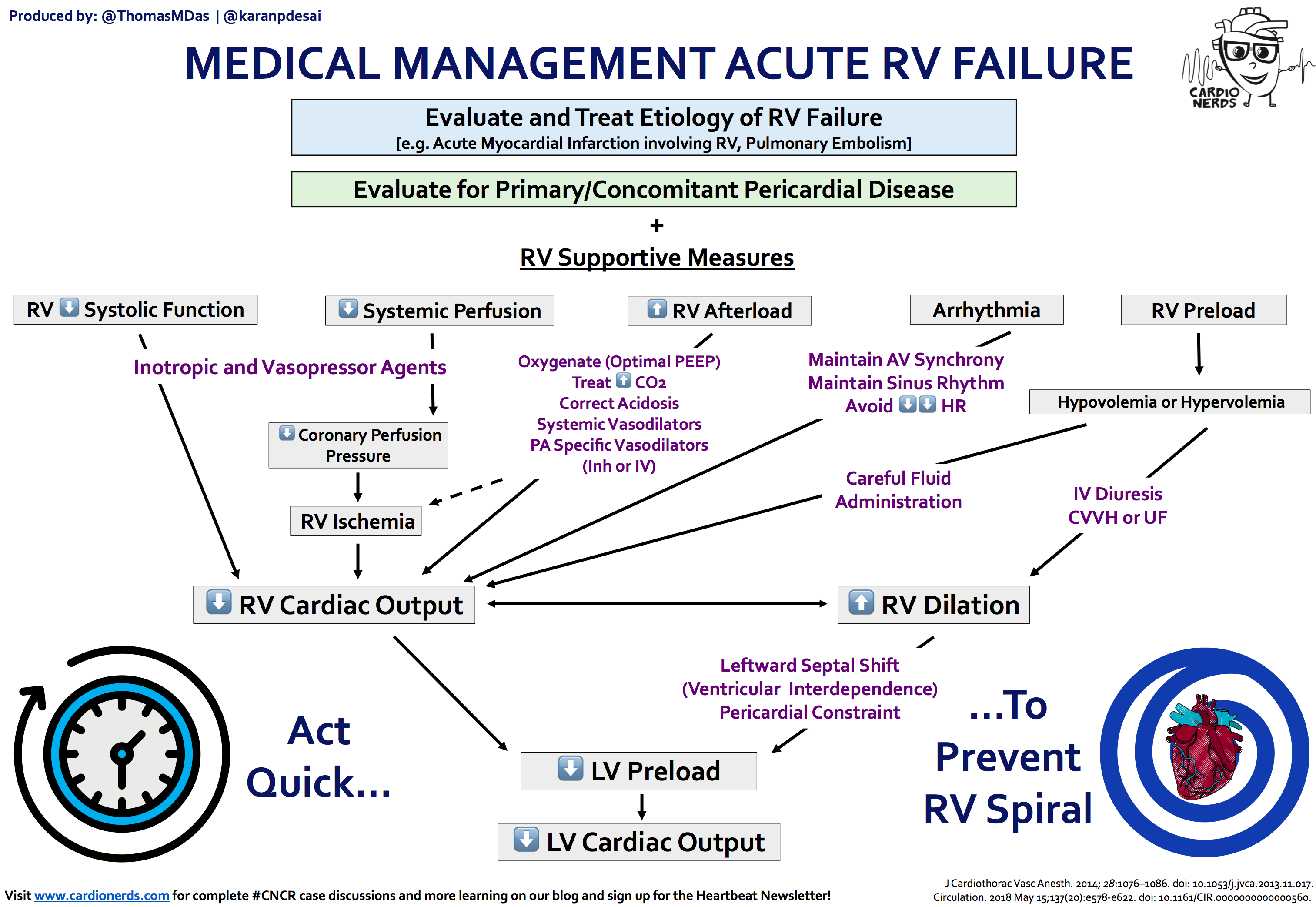
Stephanie, what happened next with the patient? Yeah, so at this point, we're in the CCU. We know that the patient clinically has sclerogenic shock. We have defined the hemodynamics, and the lab work is suggestive of shock with... worsening renal failure, elevated LFTs, lactic acidosis. He was started on the vitamin O5 to support the RV. He also was started on inhaled nitric oxide to decrease the RV afterload.
He had a trialysis catheter placed for CRRT, given that he was in renal failure, but subsequently developed lethargy and had hypercarbic respiratory failure for which he was intubated. After that, he became hypotensive despite all of these resuscitative measures that we're previously mentioning, and he required escalating doses of epinephrine.
He became body cardiac again to the 50s with a junctional rhythm. And at this point, he was 22 hours after the initial intervention on the vitamin O5, epinephrine, and I know. So at this point, we were thinking about... what the next step ought to be. So basically, you've got a patient who's getting worse on your treatment. Right now, it's pretty much limited to medication. So he's on dobutamine, which is ninotrope. He's on epinephrine.
It's an inhaled nitric oxide, and he's getting worse. So what did we do next? So I think at this point, we have exhausted chemical interventions. And as Isaac mentioned...
¶ Pacing and Inotropes in RV Failure
We were thinking about now pursuing mechanical support. Yeah, so before we get there, some important things to discuss, and this is all great points, Stephanie and Peter. Heart rate's in the 50s. We have junctional bradycardia again. It's not being sustained by dobutamine. This brings up the question always, how does temporary pacing help in RV failure or our choice of inotrope? So, Peter, why don't you tell us about how the RV pacing might be helpful here in his case?
So you have to remember cardiac output is the product of heart rate and stroke volume. So in the setting of an infarct, you're going to get to a limit on your stroke volume, in which case the cardiac output is really dependent on heart rate. So in someone who's bradycardic and in shock, that's a big problem. Luckily, we live in 2020 and we have a lot of options for improving that. The easiest and quickest way at the bedside would first be to give medications.
Things like atropine, that's usually not effective and not a long-term strategy. Next, you could go to things like medications like dopamine or butamine, things that sort of speed up conduction and speed up the heart rate.
Although a lot of times in an infarct, that also won't work. So a lot of times what we end up doing is putting in a temporary pacemaker. This is usually, you know, it's a bedside procedure or you can bring them to the cath lab to do it. A lot of times it's done at the bedside in the CCU.
In the meantime, before you can get a temporary pacemaker, if they're really in shock and they're very bradycardic, you can transcutaneously pace them. That's also not a great long-term option for a lot of patients, especially obese patients. Patients with COPD have increased enteroposter diameter of their thorax. You essentially have to get in depolarization or capturing the heart from the surface or the skin.
But that's a good temporary measure while you're getting ready to put in a transvenous pacemaker. In this case, we were able to get a transvenous pacemaker into the right ventricle and increase the heart rate, which actually did help the cardiac output.
Yeah, so that's great with getting the heart rate up. And especially with RV failure, you don't want patients to be in any arrhythmias. So if they've developed like SVT or atrial fibrillation, you'd think of early cardioversion. Now this backs the question. So we still have a swan-gens catheter in him. You know, what are we targeting here?
There's a recent study from 2019, it's also part of the National Cardiogenic Shock Initiative, showing us that in patients with AMI cardiogenic shock who develop RV dysfunction, achieving a cardiac power output of more than 0.9 or a PAPI of more than 1. within 24 hours is actually associated with higher survival by more than 80%. So this brings us to the topic of inotropes and RV failure. Are they all the same difference?
So this is a very tricky situation. The RV is coupled in sears with the left ventricle. As RV failure progresses, interventricular septumbulges to the left impairs left ventricular filling, as well as reducing the septal contribution to RV contractility.
This unfavorable left-sided septal shift leads to hypertension, reduces cordial perfusion pressure, further exacerbates the situation with more RV ischemia. For inotropes, a low-dose dibutamine has been shown to restore RV pulmonary artery coupling.
and cardiac output better than norepinephrine because of its more pronounced inotropic effect. And given that's an inodilator, it's obviously preferably used in normal-tensive patients, but sometimes we don't have a choice. We have to use it in hypotensive patients. And then you have milrinol.
a selective PDE3 inhibitor. It slows intracellular cyclic adenyl phosphate, adenosine monophosphate metabolism and improves inotropy and facilitates pulmonary vasodilation. So very attractive agent in pulmonary hypertension.
Also, in normal intensive patients who are already on chronic beta blocker therapy, it will be preferable to start melanin and then butamine at the outset, if they can tolerate it. Then you have dopamine, which we talked about improves heart rate. Dopamine also improves RV contractility.
And at doses below 16 micrograms per kg, actually increases cardiac output without increasing pulmonary vascular resistance. And then other choices are your epinephrine, which has been shown to improve cardiac output without detrimentally affecting the PVR as well. And then you have norepinephrine, which causes vasoconstriction via the alpha-1 receptor stimulation and has limited beta-1 inotropic effects. So it might not be as effective in increasing the RV inotropy in this situation.
So the long story short, overall, from experience and from preference for acute RV failure, dobutamine is the first go-to if pressures are borderline, plus minus vasopressin, which is another primary vasopressin-resistant neutral vasopressor. Milrinone, if I have blood pressure room to play with, and then where hypotension is more severe, adding epinephrine would be my next choice.
I tend to avoid dopamine if I can. I find it's a very dirty drug, causes a lot of arrhythmias, and I find it doesn't necessarily provide the same level of support. as the other inotropic agents that I mentioned. And then finally, phenylephrine should be avoided at all costs because it causes a lot of vasoconstriction and increases your primary vascular resistance and RV afterload.
¶ Early Mechanical Circulatory Support
But now we have here, you know, a patient on butamine and escalating epinephrine. So do we go to mechanical support? Do we have any data for this? And if you go way back to 1999, and there's a study by Samuels, we learned that... Hospital mortality correlates with the number and level of inotropic support necessary to separate from cardiopulmonary bypass following open-heart surgery. And with a low-dose inotrope, mortality is about 3%.
But this increases to 21% with a high-dose inotrope, just one, and up to 42% with patients on two high-dose inotropes. And from more recent data from the CVET registry from 2017, they showed similar trends. with the minor difference that even one inotrope can increase mortality by up to 54% in patients. But this time, the patients that were studied were patients who had cardiogenic shocks from acute myocardial infarction.
So basically, this suggests that we should pursue early mechanical support now that we have that option available to us. And as well, clearly here, the inotrope is not sustaining the patient, so you want to avoid even more medicines to create more wall stress and dysrhythmias. But remember also that every device has a price. So Isaac, great teaching there.
¶ Right Ventricular Assist Device (RVAD)
Coming back to our patient, you know, it can be confusing. There's so many mechanical circuitry support devices nowadays. How did you choose? Which one did you choose? What's the sort of the thought process there? So we already decided that the patient, you know, had isolated RV failure, didn't need LV support. So we don't want to think about LV support devices like Impala CP or Balloon Pop, right?
Now VA ECMO would have supported the RV, but at the expense of increasing LV after load, and he did not really need biventricular support. His LV was fine. And ECMO, as we know, is not without many complications. So we're down to percutaneous options here that include the Impella RP and the ProTech Duo. Just in general, institutional preference is real. It depends on what the staff attendings are comfortable with inserting and managing. So it could be different in your institution.
But over here, we have preference for the Protek Duo. And this is actually a temporary RVAD that's placed in the right internal jugular vein and capable of providing up to 4.5 liters of flow. And the way it does this is it's a novel dual lumen cannula. So it's inserted percutaneously via the right internal jugular vein most of the time to provide what is really a right atrium to pulmonary artery bypass.
The proximal inflow lumen is positioned in the right atrium, and the distal outflow lumen is positioned in the main pulmonary artery. And these lumens are connected to a tandem heart pump. provides the flow of up to 4.5 liters a minute, so basically your entire product output. If needed, you can introduce an oxygenator to the circuit as well, but clearly you didn't need it in this case. And from the data that we know so far,
This has been used to bridge to lung or heart transplant in patients with acute myocarditis with isolated RV failure, as well as post-LVET insertion patients with RV failure. And it's been shown to be safe and effective for short-term RV support in isolation or...
in certain cases with other LV support devices for biventricular support. So that's all very exciting for us. So Isaac, it sounds like there are a lot of devices, but you hit the nail on the head. You have to decide, are you supporting the RV? Are you supporting the LV?
Do you need to support both? And that really is going back to our swangans catheter. That's really why you need a swangans catheter in the ICU when you're differentiating these shocks and classifying these cardiogenic shock patients. Also, you pointed out that...
There might be more than one device that could do essentially the same job, and some of it will come down to institutional preference, what people are familiar with using. Besides the proceduralist putting in these devices, you also have to remember... There's intensivists who are going to manage these overnight or cardiology fellows. The cardiac ICU nurses need to know how to be trained on how to monitor these devices. So it really is a complex decision and there's a lot of devices out there.
But you hit the nail on the head. You have to decide if you're supporting the RV, you're supporting the LV, or you're supporting both, and what would be the pros and cons of each device. Yeah, and I totally agree with you guys. I've really grown a preference for the Protect Duo in certain circumstances. And in addition to thinking about which side, which ventricle we're supporting, we also think, do we need pulmonary support?
and oxygenation is particularly relevant for RV failure because the cause of RV failure is hypoxic lung disease, whether it's ARDS or another etiology where you get hypoxic vasoconstriction and increased afterload on a... otherwise normal or otherwise already failing RV. And so the benefit of the Protect Duo is the ability to attach an oxygenator. And so you can essentially get full gas exchange in addition to RV support.
As well as the fact that since it's going into the right IJ, you can also start ambulating these patients. And if they need longer term support, you can start thinking about physical rehabilitation while you're supporting them. So a lot of benefits to consider. A really awesome choice for this particular patient in general.
And really highlights what makes it so interesting and exciting to be in the field of cardiology because cardiac shock is so complex and so heterogeneous and using the tools that you have, which you're already using from the second you got called to this patient.
right you got called to the patient you were already using your ecg physical exam findings to isolate where the lesion is not the lesion but the break in the system and then echo to confirm and then clinical acumen to put it all together and then swan to be more precise and then the actual therapy and then the response to therapy.
all really goes to what makes cardiology so much fun and really allows us to apply all the cerebral ethics of what we've been trained to directly impact the lives of the patients that we have. So this really highlights that to me.
¶ Patient Recovery and Follow-up
So Isaac, now we pulled out the big guns. Now we've got them on mechanical circuitry support, temporary mechanical circuitry support. It was RV. Stephanie, what happened with the patient? Within hours, actually, he was able to be weaned off of epinephrine. And within a day, the patient started turning around the corner. His renal function started improving. He started making a little bit of urine. His shock liver started improving. His cardiac power was...
increasing up to 0.86. He's liked it clear, and his hemodynamics started improving overall. Within six days of having the ProTech Duo, The decision was to remove it, and the vitamin was eventually weaned off. The inhaled nitric oxide was transitioned to flolan, and it was eventually weaned off. The urine output started to improve and he was able to come off of dialysis.
In regards to his conduction, he continued to have intermittent junctional rhythm and sinus radicardia. So he had a pacemaker place bar to discharge. Overall, after a 27-day admission and six days on protect dual support, he was able to be discharged to rehab. And at follow-up, he is...
describing NYHA class 2 symptoms without any significant limitations. His RV function has near-normalized on repeat echocardiogram, and he remains angina-free, on-carbiterole, dual antiploidal therapy, and CRESTOR.
¶ Re-Angiogram and Key Takeaways
Just to jump in here, because I'm sure the audience is going to be asking, did we shoot those coronaries again? And we definitely did when we put in the ProTech, just to be conscientious. The left system was patent as it was before, a patent left LED to D1 stamp.
There's no new lesions there. RC angiography was not to rule out stem thrombosis, which was the most important thing, which we didn't think was happening. But it did demonstrate sluggish, but functionally flowing, but widely patent coronary artery that was large and dominant like we saw before. There was no evidence of any residual stenosis or inclusion or even any evidence of any thrombus from the previously placed stents in the RCA, either in the stents or distally in the PDA or PLB.
The right ventricular branch and side branch occlusions were again noted. It was teeny one flow for him. So to summarize, we had a gentleman coming in for... worsening anginal symptoms despite maximally tolerated medical therapy. He was on a good dose of beta blocker, calcium channel blocker. He was on rinolazine and also long-acting nitrates. And despite that, he was still having chest pain.
He went for an angiogram and his culprit lesion was in the right coronary artery, which fit with his nuclear stress test. He underwent PCI of that culprit lesion and then... Post-PCI that evening, the night call fellow was called for hypotension and bradycardia. And on reviewing the cath films, we had actually, during the PCI, it occluded some marginal branches to the RV.
which normally doesn't cause problems. But in this patient, it caused an isolated RV infarct, which we saw clinically at the bedside, but as well as with our tools like our EKG showing a... ST elevation or injury pattern, V1 or V4 in his case, as well as bedside echo showing a dilated, severely depressed RV. He had worsening shock on medical therapy.
We placed a swan gans catheter to tailor our treatment decisions based on his hemodynamics. And eventually he got upgraded from essentially inotropes and vasopressors to... mechanical circuitry support or temporary mechanical circuitry support, as well as temporary pacing to improve his heart rate. Eventually, he was able to come off of his mechanical circuitry support, his shock improved.
He was able to be discharged to rehab and eventually in follow-up had no limitations. Thanks for summarizing the case, Peter. That was great. So the take-home points here is, you know, when you see something like that acute marginal. big branch. Don't always discount the side branch. So sometimes maybe a provisional stenting with the gel balloon technique might be important. And then we reviewed the EKG changes here earlier.
The EKG changes accompanying RV infarction, they vary widely. And if they're isolated, anterior segment SE elevations in V1 to V3 and up to V5 are seen, as well as in leads V3R and V6R. So it's a right set of EKG. It's important to remember, like in this case, not all shock is created equal. Your swan-gens catheter becomes important in cardiogenic shock for hemodynamics to cognitive therapy. You definitely need experience for this. So if you get garbage data in...
you're going to get garbage data out and it's useless. So you've got to do it properly. Okay. Your inotropes and your vasopressors have a cost. You're asking yourself, do your patients need mechanical circulation support? Answer is probably yes. And we should escalate quickly before it becomes too late.
You need to tailor your level of support. Is it for the LV? Is it for the RV? Or is it biventricular, where you're considering ECMO? Don't forget the RV, right, in this case. So you may forget it, but it will not forget you. The early escalation to temporary right-sided mechanical circulator support can help rescue these patients very quickly and with good outcome because the RV is very good at recovering even after many insults. We've seen this.
These patients just need support to tie them through. And while we've discussed the case today, specifically for an infarct-related RV failure, these same principles apply to RV failure in post-LVAP patients. post-heart transplant patients with isolated RV failure due to long ischemic time, isolated RV failure in myocarditis, and even in patients with severe pulmonary hypertension and RV failure. So these are all useful principles that we can make use of.
¶ The Rationality of Cardiology Management
when we take care of these different sets of patients. Guys, I love that. Don't forget the RV because it definitely won't forget you. And I've definitely been called upon by a failing RV in the past. And I personally find these to be amongst the most complicated clinical situations. For a variety of reasons. But I think the way you walked us through the management was absolutely pristine and very high level.
What I love about cardiology is that it's so rational, right? Even though the things are complicated, the situation could be, you know, blaze on fire in front of your eyes. The core principles are still the same. Here was a patient in cardiogenic shock. You used invasive human dynamics to guide your management.
And you went back to cardiac output. Cardiac output is stroke volume times heart rate. You didn't have enough heart rate and you didn't have enough stroke volume. You increased the heart rate by temporary pacing, but you also had to address the stroke volume, which was... diminished because of RV failure. And then you went to the basic core principles of improving stroke volume.
Addressing the preload, addressing the afterload, addressing inotropy, right? In RV specifically, the preload is particularly challenging because as the RV is failing, this is already a week. thin-walled, compliant ventricle chamber. And as it's failing, it just becomes more and more like a passive conduit. And so it becomes very preload dependent.
And so you have to make sure there's sufficient preload. But at the same time, if you fill it up too much, it bows out and dilates and starts impeding flow and preload within the left ventricle. And in that context, you can have decreased cardiac output because you're hurting the left ventricular output.
And so, you know, very carefully titrating the preload into the RV is so important. And this is where a Swann-Gans catheter, again, is very useful. But you have to make changes and then follow up the hemodynamic response. The afterload. Again, this is particularly important because the RV is very dependent on afterload and small changes in afterload can make massive changes in the stroke volume for the RV side. And so here you use pulmonary vasodilators.
like inhaled nitric oxide and then transition to ibuproxenol. But then also increased AFRL could be from hypoxic vasoconstriction because of a lung problem. And it can also be from excessive... positive pressure ventilation, which is also very important to consider when thinking about how to ventilate a patient with RV failure. And then we talk about inotropy.
Here, we use positive inotropes to help with inotropy. And because we weren't getting sufficient response, we moved to essentially mechanical inotropy with using Protect Duo. And then we talked about the use of VA ECMO for biventricular support, as well as a possibility of using an axial flow device.
RV in Pella. So just overall, it's a very complicated case, but you guys very rationally thought about where were the deficiencies in the hemodynamics and approached it very rationally in a stepwise manner, saving a life.
RV in particular has such a great propensity to recover after an acute insult. So you essentially took the patient through this acute insult, saved the life, and the patient is doing well. So really, congratulations on taking tremendous care of this patient through a very complicated...
situation. Yeah, Amit, you took the words right out of my mouth. And by the way, say hello to Drew for us. We love him so much. Could you hear him crying in the background? I'll have to give him a hug after this recording is done. Yeah, yeah, Andy, if that fits with your parental mission. I totally agree. You know, foundational building blocks, which we just really demonstrated, is the real key to success with resuscitation in the most...
¶ Houston Methodist Fellowship Experience
And that's really what makes my heart flutter about cardiology. But Isaac, Stephanie, Peter, why don't you tell us about what makes your heart flutter about cardiology and particularly with training at DeBakey? I guess I'll start. I was looking for clinically heavy training when I was finishing up my residency. But what really blew me away here, drove me to Houston Methodist, was during my interview day. I met some of the most kind and approachable faculty.
no matter what their reputation might be. Being in the heart of Texas Medical Center, our fellowship offers a breadth of exposure like no other. Everything's under our umbrella of the cardiology department, cardiac CT, cardiac MRI. We read all those. We have a lot of transplants coming in and out. We see rejection. We see acute MI. A lot of mechanical support, which is what really attracted me as well because I have a huge interest in that. So intrauteric balloon pumps, impella and ECMO.
We have everything we need to provide the best care for our patients and I guess the best training for our fellows as well. It's very clinically robust. We'll train the best general cardiologist there is, but it will also show you what... your next steps could be, and that's exactly what I experienced. We have both the right faculty and the right equipment to help you to succeed, and certainly no shortage of cases, as the call volume would realize.
Really, what makes it such a joy to work every day is our faculty treats the fellows like junior partners and colleagues. I called Dr. Hussain and Dr. Bimraj overnight to discuss crashing cardiogenic shock patients, as we did for this one. whom we think we need to escalate to mechanical support. Or I can call Dr. Alpesha or Dr. Neil Kleinman to discuss high-risk NSTEMIs that need to go urgently to a cath lab, or even Dr. Huey Lin for all the Fontan patients who come in overnight.
who don't know their past middle history, and it's like a fact-finding mission at 3 a.m. So it's clear that the faculty are genuinely excited about fellow education and share our goal for providing excellent patient care. So that's all very exciting.
But more importantly, I think as a fellow that's applying, are you going to be trained well enough by the time you finish this? And so by the end of your second year of training, by the end of my second year of training, you'll be able to comfortably handle... a large range of complex cases. And this includes, but it's not limited to, you know, running the cardiac PET lab with Dr. Almala, insertion of emergent bedside intra-aerotic balloon pumps, which Peter and I have done.
perhaps too regularly, fortunately, for patients in cardiogenic shock or just running the cardiac intensive care unit as an intensivist during the COVID-19 pandemic. And in the CAF lab, we scrub in as primary operators, help with impeller insertions. We help with PCI all the time. It's great training. We are a tightly knit and diverse group of fellows. We are from all over the world. There's people from Lebanon, people from Syria.
I'm from Singapore, and our faculty as well is from all over the world, and they're all renowned. And they're such a pleasure to work with. It's crazy to think that I do my clinic every Tuesday with Dr. Zagby. He needs no introduction. but they're all so humble and also kind. This is like my second family. If I had to make a choice again, I would definitely come here. It's an easy answer. What about you, Peter? What do you think?
Yeah. Thanks, Isaac. I've always been interested in cardiology going back to medical school, just cardiac physiology. And then as I got more interested in that, I learned more about electrophysiology and residency. And that's what... got me interested essentially in coming to Methodist. When I was interviewing, I knew I wanted somewhere that would have really broad cardiac training. And I think you really get it at Methodist at DeBakey here because...
We do everything advanced, and that leads to getting broad clinical training. So we have a pretty robust transplant program, VAD program. We have a really active cardiac ICU. Everything that's cardiac imaging, so cardiac MRI, cardiac CT, all of that is under the cardiovascular department. So we get a ton of exposure to these advanced imaging techniques, advanced heart failure, transplant, and then EP.
really goes along, advanced EP stuff goes along with your advanced heart failure. A lot of your VT ablations are the same patients who are being evaluated for an LVAD or evaluated for a transplant. If you want to get experience in...
advanced EP, like VT ablation, epicardial ablation. We also have one of our attendees, Dr. Valverano, is an expert in venous alcohol ablation, not just of AFib, but also of VT. He's kind of pioneered a lot of... work in that space so i've had a great experience here i would definitely come here again like isaac said i'm basically friends with all my co-fellows which is you know makes work a lot easier when you can basically you're just working with your friends every day
So yeah, I've had a great time here. How about you, Stephanie? Yeah, so my experience is a little bit different in that I was already a resident here. So I had the benefit of knowing the program a little bit more. And I obviously, you know, loved Houston. It's a multi... cultural city with lots of opportunity. The medical center is the largest in the world and you have many different fellowships here. But throughout the interview trail, I always kept comparing back to Houston Methodist.
I realized that the program had pretty much everything that I wanted out of a fellowship. Peter and Isaac have brought up the collegiality is huge. Within our co-fellows, we help each other through the whole process. First year is obviously very clinically heavy. We're challenged with all these complex patients, but we also have the support of our staff.
It's important for me because I was pursuing electrophysiology and in order to get the exposure of the most complex electrophysiology procedures warrants complex patients. not just from heart failure patients, LVAD, transplant patients, but also congenital patients doing pacemaker implants in this complex anatomy is fascinating. And this program provides all of that. So to sum it up.
It's a very clinical heavy, supportive, diverse, and I think fellows that complete this program will receive a very well training overall. pretty good environment that it's important to have in a challenging fellowship like cardiology is. And one more thing I forgot to say about Houston, because I didn't know as much about Houston as like Stephanie, for example.
It is such a culturally diverse city. The food scene is amazing here. I really had no idea until I moved down here, but there's just like world class, like all different kinds of cuisines. And it's been really fun. someone who likes that to go out and eat at all these new restaurants. Isaac, Stephanie, Peter, thank you so much for walking us through this incredible case. You've certainly elevated us with your teachings and discussion points.
as well as your passion for education. And I'm sure you've made with this episode and all the work you do, everyone over there at Houston Method is very proud. Thanks again for spending your Sunday of Labor Day weekend with us. This was absolutely fantastic. We'd love to have you back on later and we'd love to visit you all to...
¶ Expert Perspective: RV Failure Etiologies
test out the food scene sometime down the road. You're welcome. Thank you for having us. And now for our eCPR segment, I want you to introduce Dr. Mawash Kasi. She's an advanced heart failure attending here at Houston Methodist Hospital. Dr. Kasi? Hi. Thank you for inviting me to this session. Isaac, Stephanie, and Peter, you guys did a great job, as always.
I must say, I'm very lucky to be part of a fellowship program where when presented with patients who have cardiogenic shock, my fellows put in the SWAN catheter and call me with numbers and tell me that they've done X, Y, and Z, which is exactly what kind of happened in this situation. I must also add that I have a newfound respect for the RV marginal branch because this is a very unusual case where somebody had PCI and the RV marginal branch went down and then we saw profound RV failure.
So the way I like to think about RV failure whenever I'm in a situation where the SWAN numbers are all pointing towards RV failure is to recognize which anatomical part of the right ventricular system is affected. Is it the pump, meaning are we dealing with myocardial ischemia or are we dealing with myocarditis? Or is it the valve issue, meaning that the tricuspid valve is incompetent and is causing volume overload?
is it the conduit issue by which whether there is pulmonary vascular resistance that is high because of pulmonary hypertension Or is it a true mechanical obstruction, such as in cases of pulmonary embolism? Or is it due to the septal interaction, which is, of course, the bane of my existence as an LVAD cardiologist, where we see a lot of suction right after an LVAD surgery, and that results in...
RV failure. So, of course, when you know what the problem is and which anatomical portion of the RV you're dealing with, if it's pump failure, obviously inotropes. Pacing does help, and that was actually the situation in this case. and where if we did go up on the heart rate, the patient's maps improved. Then it's very important to optimize the preload and RV afterload.
Meaning if the patient has a CVP above 15, it's important diures. Whereas if the patient's CVP is very low, it's important to maybe load the patient with some volume because as we know that RV is dependent on some preload as well. Then any kind of pulmonary hypertension related issues should be triggered to use nitric oxide early.
¶ Management of Refractory RV Failure
Now, in this situation, the patient was already on inotropes. The pacemaker was inserted. Nitric oxide was started. And despite all of these interventions and use of vasopressors, the patient still was in refractory RV failure. And that is exactly where the next step should be to consider right ventricular assist devices.
Now, there is a definition of persistent or resistant RV failure, and that is when you have somebody who has a cardiac index that is persistently low despite using inotrope dosages, usually dibutamine greater than 10. We usually don't do that. in the equivalent dose for almost 120 minutes. And in addition to that, if you have a persistently elevated CVP, by echo if you have RV dysfunction, or if you have an RA to wedge ratio or in PAPI that are unfavorable.
In this situation, the device that you could use is really a lot of times institutional preferences. In our institution, we're pretty open to both using surgical and non-surgical devices. By surgical, I generally mean Centromac. In some institutions, they do not use percutaneous devices, so Centromac is the go-to device.
Whereas the percutianics devices include Impella, the Tandem, and Protec Duo. My personal preference usually is Protec Duo because, of course, of the ease of converting it into an oxygenator if need be.
And then the importance of early ambulation because we know that this goes through the right internal jugular and the inlet is at the RA, the outlet is at the PA. So it's actually a very neat device and it is easily implantable, both surgeons and... cardiologists can do it and then you can ambulate your patient while letting them recover.
One of the other nuances that I wanted to go over in terms of RV assist devices is that you have to think about what will happen next. Is this device a bridge to recovery or do we have an exit strategy? In this situation, of course, we were hoping for recovery. and which is what exactly happened. And then once you have inserted the RV assist devices, important things to think about is what is my candela position? Where is the inlet and where is the outlet? Because it's important to realize.
and daily monitoring where the inflow and the outflow candelab positions are. And then the other important thing is anticoagulation. A lot of these or all of these patients have to be on heparin and have to be appropriately anticoagulated. There is a risk of both bleeding and stroke, which is not insignificant in these right ventricular assist devices. So you could either have a circuit that...
directly bypasses the RV, such as the Protec Duo, where the blood is bypassed from the right atrium into the PA. Or you could have an indirect right ventricular bypass, which is usually ECMO system, where it completely bypasses the heart and you have a certain... that generally keeps the patient alive. While ECMO is the last resort for these patients, you want to have a device which basically unloads the right ventricle and allows it to recover if it is being used for a recovery strategy.
Now, a few of the other important things is to understand what this right ventricular assist device is doing to your left ventricle. So understanding the hemodynamics and how they're impacting the left ventricle is also important and should be a very important part. of the consideration of what you would do or would use as your go-to device in that situation.
Now like I said earlier, not all right ventricular failure is the same. So you can't just use a device for any type of RV failure. For instance, if you have somebody who has pulmonary hypertension, I do not think the way to go is to an RV assist device because the RV assist device may not be able to unload appropriately if the pressure is too high in the pulmonary vasculature. Rather, it would be beneficial to use nitric oxide in those type of situations.
In conclusion, important to realize what is the etiology of the RV dysfunction. And if all the steps are done, inotropes, optimizing preload and afterload, optimizing the rhythm, the next step is to consider right ventricular. assist devices and then impact off that right ventricular assist device on the left ventricle. Thank you so much.
¶ Program Director's Message
And now for a few words about our program, Dr. Stephen Little, who's our program director and one of our stellar imaging attendings. Hey, Cardio Nerds Nation. This is Stephen Little. I'm the program director for... core cardiology training at Houston Methodist. I'll just take a second and say just a little bit about Houston Methodist as a cardiology training center. So we are in the heart of the Texas Medical Center. Houston Methodist is a large hospital.
About 800 beds currently ranked number 12, U.S. News and World Report for heart and vascular care. I think some of the things that make us unique for our training program is that we're a large training center with a lot of fellows under one roof. So we take six fellows a year times three, so that's about 18 core fellows. But we also have a lot of subspecialty fellows, three heart failure, two EP, two interventional, structural.
four to five imaging fellows, postdoc fellows, research fellows, all under one roof. So it sort of makes for a really neat training environment to have all these different levels within one space. Core training is pretty standard first and second year. One of the unique features for us is that we really provide a lot of elective time. The luxury of having all those fellows under one roof is that the clinical service is sort of front-loaded in the first year.
And the second and third years have a lot of elective time. So creating opportunities to focus on imaging or research or intervention. achieving level three, for example, in an imaging modality or all of the cath cases you need to feel comfortable before you start your structural fellowship. These things are opportunities that Houston Methodist does before. I think currently right about 14 months of elective time.
the core 36. And that's pretty unique across the country. We're academically also very busy. I don't know the exact number, but we're multiple hundreds of publications per year. by the faculty and fellows at Houston Methodist alone. So it's a busy academic center, a busy clinical center, but there's absolutely time for fun. COVID has put a little bit of a kibosh on the stuff we like to do.
But we have an annual paintball event where we get together with surgeons and try to shoot each other. And that's usually kind of fun. We have meet and greets and mentoring sessions. I do encourage you to go to our website. It's really pretty good. Go to the DeBake Education website and see some of the archived lectures that are freely available to all of us, all of you. And consider Houston Methodist, both for your core training, but also for your subspecialty training.
If you've never been to the Texas Medical Center, or even worse, if you've never been to Texas, you really do have to come and visit. So if you're sick of winters and you really like to come and visit a place that I think has truly outstanding cardiac training. consider Houston Methodist. Thanks. And thanks to Isaac for the invitation.
What an amazing episode. A huge thanks to the fellows and faculty for enriching us with another terrific discussion and an incredible addition to the CardioNerds case report series. Be sure to check out the show notes for all of the case media available for review, key take-home points and discussion points, and links to the program. If you'd like the educational takeaways and graphics delivered directly to your email, sign up for The Heartbeat, the Cardio Nerds newsletter.
by clicking on the link in the episode show notes. We thank the ACC Fellow in Training section chaired by Dr. Nosheen Reza for their incredible support and collaboration. And a very special thanks to our phenomenal production team. For elevating the platform, Colin Blumenthal, Tommy Das, Eunice Dugan, Rick Ferraro, Evelyn Song, and Vivian Verghese, internal medicine senior residents at the Johns Hopkins Hospital, as well as the team med ed mentor and University of Maryland.
cardiology fellow karen desai if you love the show as much as we do be sure to spread the word read and review us on your favorite podcast platform and consider becoming a patron of the show on patreon all right that's a wrap time to make like an s do and split